Last week Misha taught us about different types of housing provisions that are available for various populations who are experiencing homelessness. One of the biggest myths surrounding homeless response is that Housing First provides no oversight and is a failure. The idea that some of us could be working so hard to keep a roof over our families heads, while others in our community are living in swanky homes for free, could feel really upsetting. Fortunately, this myth is just not true.
Housing First is an evidenced based principle that housing providers follow to ensure the most success for households transitioning out of homelessness. The data shows– it is successful. In fact it is 88% more effective than failed ‘Treatment First’ models, which previously required individuals to show themselves to be ‘housing ready’ before placement. 79% of participants in housing first programs remained stably housed 6 months later. In addition, participants are less likely to use substances, and are more likely to engage in services. Housing First is a kind of Harm Reduction which acknowledges that the only way to end homelessness is to provide a home.
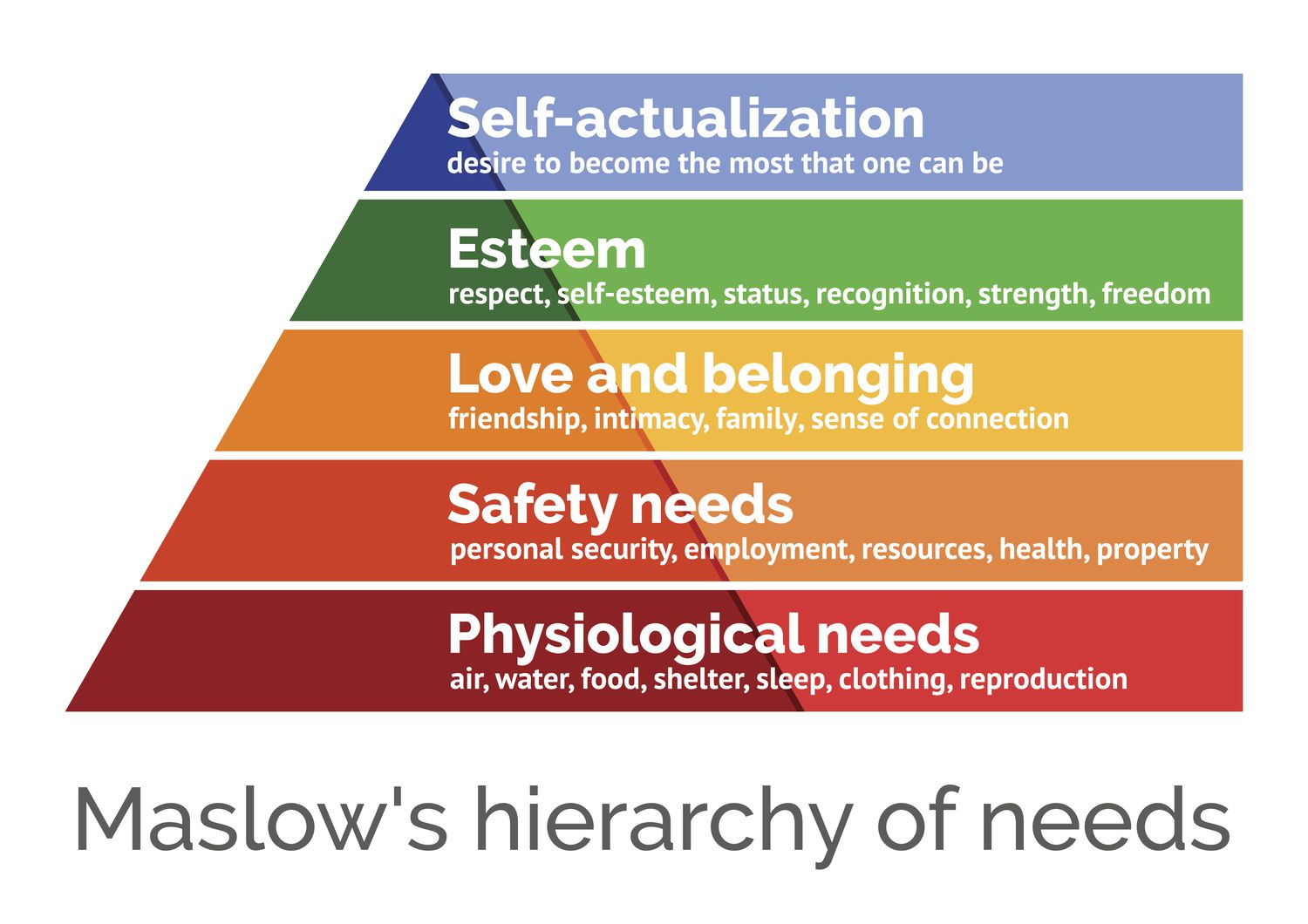
The reason these programs are so successful is a basic understanding of human need. Engaging in health, mental health, and substance use disorder treatment requires individuals to be in the correct emotional and physical state. Abraham Maslow theorized that all behavior is motivated by 5 basic categories, demonstrated in a pyramid. The Maslow hierarchy of need has been a cornerstone in mental health care and social services since 1943. The pyramid starts with concrete physical human needs- food, shelter, sleep. Only when those needs are met can people be motivated by more ambiguous concepts like employment, connection, and the desire for self improvement. Housing First allows people to first meet their basic human need for shelter, food, and safety before moving into higher needs. It allows them to take a deep breath with one thing handled- a warm bed. Then housing providers surround that individual with services to help them achieve their other goals, including healthcare, sobriety, and income.
Housing First is infused throughout all US Department of Housing and Urban Development (HUD) programming and is considered a best practice in service provision across the United States. It takes away the presumption that social workers and program staff know what is best for the client, and instead returns that power to each person, where it belongs. Housing First is not just found in the US. In fact It is infused in homeless response all over the world, including in Canada and the UK. There are five key principles of Housing First:
- Immediate access to permanent housing with no housing readiness requirements. As discussed, Housing First acknowledges that simply by being a human that is alive, every person is ‘housing ready’ without any other qualifiers.
- Consumer choice and self-determination. No one wins in a power struggle trying to force people into a pre-described course of care. Instead, wrap-around services help motivated clients to make the best decisions about their own needs for themselves.
- Recovery orientation. Housing First provides all the elements individuals need to foster safety, without requiring abstinence. Participants will have access to a variety of social, emotional, educational, occupational, and other services and activities to encourage them to be full community members.
- Individualized and client-driven supports.Housing First avoids a ‘one-size-fits-all’ approach and instead allows clients to drive their care plan. Some individuals or families may only need short term support, while others may need a higher level of care.
- Social and community integration. People experiencing homelessness have often been pushed to the margins of our community. Housing First recognizes their dignity and worth and explicitly names their value to our communities.
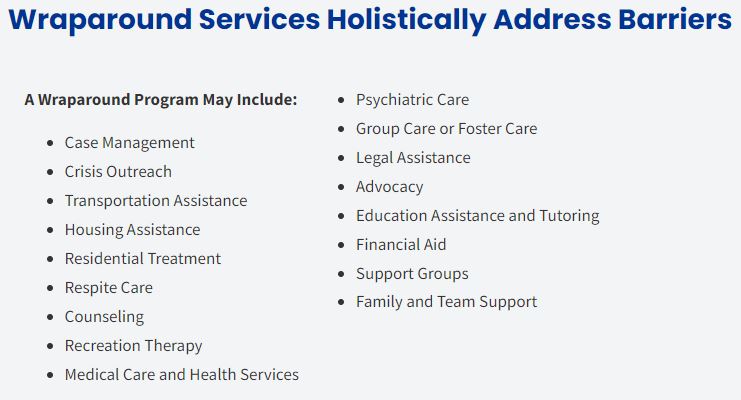
Housing First does not mean housing only. HUD service providers offer ‘wraparound’ services. This is a coordinated approach between health and mental healthcare providers, education and job placement, public assistance, transportation, and more to support the experience and recovery of the individual. As households transition out of homelessness, they have a variety of needs. Many need to heal from trauma before or during their time unhoused. Most need help finding employment or increasing their wages. Jeff Olivet, executive director of the U.S. Interagency Council on Homelessness addresses a group of county leaders in July 2023. He was very clear: “all of those wraparound supports are what keep people housed … the real recipe that we know works is a combination of housing and services, it’s not ‘either or.” Wraparound services are team based. The types and level of services in each case is determined by case workers and the participant together.
Housing First programming works in all the metrics we evaluate for success in public policy. Housing First immediately lessens the taxpayer cost of homelessness saving over $15,000 per year per consumer in emergency services and costs up to $23,000 less per year than shelter programs. A 2004 study in the American Journal of Public Health showed participants in Housing First programs got housing sooner, stayed housed longer, and engaged in services at a higher rate than participants in a treatment first model. A 2009 study published in JAMA (a highly respected medical journal) found that even when clients with alcohol addictions did not choose to participate in treatment, formerly homeless participants in a Housing First model program still reduced their alcohol intake over time. Housing First is shown to reduce violence in families who have experienced domestic violence and improve health outcomes for those living with chronic illnesses like HIV/AIDs. Pathways to Housing in Philadelphia is reporting that 65% of their participants with Opioid Use Disorder seek treatment after joining their Housing First program.
We also know it works because the process for funding insists that programs are successful. HUD program dollars are administered by local Continua of Care (COC) agencies across the country. There are 8 COC agencies in Missouri. Each COC annually reviews the grant funding of the agencies within their geographic area and determines which programs should continue to get funding and which might be eligible for reallocation of funding. New programs also have the opportunity to explain their ideas and plans and compete to receive funding. These programs are reviewed by community members who do not work for any of the agencies up for funding and are evaluated on similar metrics. These metrics include increasing income, connecting clients to health and mental healthcare, and evaluating drug and alcohol treatment participation. Unsuccessful programs are likely to face funding reallocation, where a portion of their funding is offered to either higher performing or new programs.
I disagree with many of your statements and your data is flawed. you only have to look at numerous Democratic social programs in San Francisco. nre York, Chicago. Denver to mention only a few. while your ideas sound good. in mo we have practically no mental health services for the chronic ill. without great supervision putting sick people in an unsecured environment isn’t safe for anybody.
They literally backed up their statements with evidence, unlike you.
What do you do if the homeless person refuses to leave for help because of his mental health and I have tried everything. He’s living in my driveway in his car and doing other things I can’t mention here
well remember be patient and ask yourself what would Jesus do